A Funny Turn On Thursday
Because of my endoscopy at five on Thursday, I had a quiet day. I wasn’t allowed to eat anything for eight hours before or drink anything but water for four hours.
About one in the afternoon, I was sitting at my computer, typing a post into my blog.
And then everything, went rather fuzzy and words were coming out garbage. Often each letter was replaced by one of the next on the keyboard.
I was also a bit unsteady on my feet and as I was alone in my house, I decided to go out, so that if it was something worse and I collapsed, there would be someone to help me.
As I got to the bus stop, which is about fifty metres away, a violent thunderstorm broke out.
On the bus to The Angel, I tried to check my phone to get the time. It didn’t respond and I couldn’t unlock it. And even with help from the EE Shop and a guy on the bus, the phone wouldn’t respond to my fingers.
At the Angel, I did at least have a sensible conversation with an assistant about a clothes purchase, but in the end I bought nothing.
I left the Angel earlier than I’d intended and as I was on a 38 bus, which starts my journey to Homerton Hospital, I gave up on the idea of going home for some water.
I had a long change at Dalston Junction for the 242 bus for the hospital, but at least the rain had stopped somewhat and I was by now steady on my feet.
My phone was also working, so I was able to read the instructions about where to go at the hospital.
So what had happened to me at one in the afternoon?
Was there a low pressure before the storm, that sucked all the water out of my body and in the process made my fingers dry, so they didn’t work the phone?
Interestingly, I lost 0.9 of a Kg between 08:00 on Thursday and 08:00 on Friday. Was that just the fasting?
My INR also dropped from 2.4 at 08:00 on Thursday to 2.0 at 08:00 on Saturday. Was that because of all the fluid I lost, thickened my blood?
I Had My Fifth Endoscopy Yesterday And The Fourth Without A Sedative!
After two at Addenbrooke’s in Cambridge, this was my third endoscopy at Homerton in East London.
The most difficult part was not eating for eight hours before and only drinking water for four hours before.
I have mild anaemia and they were looking for cancer.
Luckily for me, they didn’t find any.
I did however lose nearly a kilo in weight.
Was that the diet or the long walk to the bus, which took me home?
Endoscopies At Homerton
On their information, they sent me, Homerton said they prefer to do endoscopies without a sedative.
I suppose it is more efficient, as Addenbrooke’s told me nearly thirty years ago.
Conclusion
I am certainly not worried about endoscopies and if your doctor says you have should one, make sure they talk you through it sensibly.
Years ago, I was on holiday in Capri and met a party of about six American gastroenterologists, who were horrified, that I had had two endoscopies without anaesthetic.
But then, I think they were more worried about the fees, that the anaesthetist didn’t get.
When Homerton investigated my gallstones, I said I’d be happy to undergo the procedure without a sedative, although, the specialist private surgeon, doing the procedure for the NHS, was accompanied by an anaesthetist. In the end the anaesthetist just stood by, in case he was needed and the surgeon did his first endoscopy without a sedative. He was very pleased with everyone’s performance including mine.
Appropriate Nutrient Supplementation In Coeliac Disease
The title of this post, is the same as that of this article on PubMed.
I choose this article, as the abstract gave a good list of related problems to coeliac disease.
This is the abstract.
Reduced levels of iron, folate, vitamin B12, vitamin D, zinc, and magnesium are common in untreated celiac disease (CD) patients probably due to loss of brush border proteins and enzymes needed for the absorption of these nutrients. In the majority of patients, removal of gluten from the diet leads to histological recovery and normalization of iron, vitamin, and mineral levels. Iron deficiency anemia is the most common extra-intestinal sign of CD and usually resolves with adherence to a gluten-free diet. However, deficiencies of both folate and vitamin B12 may persist in some patients on a gluten-free diet, thus requiring vitamin supplementation to improve subjective health status. Similarly, exclusion of gluten from the diet does not always normalize bone mineral density; in these cases, supplementation of vitamin D and calcium is recommended. Resolution of mucosal inflammation may not be sufficient to abrogate magnesium deficiency. Since gluten-free cereal products have a lower magnesium content as compared with gluten-containing counterparts, a magnesium-enriched diet should be encouraged in CD patients. In this article we discuss the frequency and clinical relevance of nutrient deficiency in CD and whether and when nutrient supplementation is needed.
I am coeliac and was diagnosed at fifty, by by a mixture of the suspicions of an elderly locum, the very modern genetic test and the classic endoscopic test , in the last few years of the twentieth century.
I have to admit, that being diagnosed was a bit of a surprise.
Application Of Control Engineering Principles To The Calculation Of Pharmaceutical Drug Doses
Today, I was asked by an eminent cardiologist to give my opinion on this scientific paper in the Journal of the American Heart Association, which was entitled Personalized Antihypertensive Treatment Optimization With Smartphone‐Enabled Remote Precision Dosing of Amlodipine During the COVID‐19 Pandemic (PERSONAL‐CovidBP Trial).
This was the background to the study.
The objective of the PERSONAL‐CovidBP (Personalised Electronic Record Supported Optimisation When Alone for Patients With Hypertension: Pilot Study for Remote Medical Management of Hypertension During the COVID‐19 Pandemic) trial was to assess the efficacy and safety of smartphone‐enabled remote precision dosing of amlodipine to control blood pressure (BP) in participants with primary hypertension during the COVID‐19 pandemic.
These were the methods and the results.
This was an open‐label, remote, dose titration trial using daily home self‐monitoring of BP, drug dose, and side effects with linked smartphone app and telemonitoring. Participants aged ≥18 years with uncontrolled hypertension (5–7 day baseline mean ≥135 mm Hg systolic BP or ≥85 mm Hg diastolic BP) received personalized amlodipine dose titration using novel (1, 2, 3, 4, 6, 7, 8, 9 mg) and standard (5 and 10 mg) doses daily over 14 weeks. The primary outcome of the trial was mean change in systolic BP from baseline to end of treatment. A total of 205 participants were enrolled and mean BP fell from 142/87 (systolic BP/diastolic BP) to 131/81 mm Hg (a reduction of 11 (95% CI, 10–12)/7 (95% CI, 6–7) mm Hg, P<0.001). The majority of participants achieved BP control on novel doses (84%); of those participants, 35% were controlled by 1 mg daily. The majority (88%) controlled on novel doses had no peripheral edema. Adherence to BP recording and reported adherence to medication was 84% and 94%, respectively. Patient retention was 96% (196/205). Treatment was well tolerated with no withdrawals from adverse events.
These were the conclusions.
Personalized dose titration with amlodipine was safe, well tolerated, and efficacious in treating primary hypertension. The majority of participants achieved BP control on novel doses, and with personalization of dose there were no trial discontinuations due to drug intolerance. App‐assisted remote clinician dose titration may better balance BP control and adverse effects and help optimize long‐term care.
About Myself
I am a Graduate Control Engineer, who graduated from the University of Liverpool in 1968.
I then worked at ICI in Runcorn for eighteen months, before moving to ICI Plastics Division, because of the untimely death of my father-in-law.
One of my tasks at Welwyn, was to look at control algorithms for chemical plants. For this I often used a PACE 231-R analogue computer.

Note.
- These computers could solve up to a hundred simultaneous differential equations at one time.
- They were programmed by wiring the various amplifiers and potentiometers together to simulate the equations.
- There were only a few transistors in these powerful machines, as all electronics were thermionic valves.
- Two of these machines wired together, were used to calculate the trajectories of the Apollo missions.
They were the unsung heroes of bringing Jim Lovell and Apollo 13 home safely.
Determining Control Algorithms
In a typical problem, I would model the a section of a chemical plant and the control system around it.
This would then lead to recommendations, as to the design and operation of the plant, so that it performed as required.
It could be argued that the body of an animal, is a very complicated integrated chemical plant, with a sophisticated control system.
For instance, if sensors around the body, say you are slightly low on fluids, your brain determines you should have a drink.
Many control loops on a chemical plant are controlled by proportional–integral–derivative controllers, which are commonly known as three-term controllers.
This is the first two paragraphs of the Wikipedia entry for three-term controllers.
A proportional–integral–derivative controller (PID controller or three-term controller) is a control loop mechanism employing feedback that is widely used in industrial control systems and a variety of other applications requiring continuously modulated control. A PID controller continuously calculates an error value
PID systems automatically apply accurate and responsive correction to a control function. An everyday example is the cruise control on a car, where ascending a hill would lower speed if constant engine power were applied. The controller’s PID algorithm restores the measured speed to the desired speed with minimal delay and overshoot by increasing the power output of the engine in a controlled manner.
I wouldn’t be surprised that the app in the smartphone used in the PERSONAL‐CovidBP Trial contained a form of three-term controller.
These are some points about three-term control algorithms.
Changing Of External Factors
One that was the villain in a problem, I dealt with, also affects my body – the weather.
I was asked to look at the problem of a chemical reaction, that overheated in hot weather. But the plant operators solved it by better insulation and ventilation of the plant and the standard three-term controller adjusted itself automatically to the new conditions.
After my stroke, I am on Warfarin for life. I test my own INR with a Roche meter and I have noticed that atmospheric pressure affects my INR. I change my deose accordingly, using a simple algorithm, of my own design.
The More You Test The More Precise The Control
If you take the cruise control example used by Wikipedia, speed is monitored continuously, as I hope, it would be if you were driving yourself.
But obviously, in many systems, where you are using an input with discrete values to control a system, you can’t be as precise as the data you collect.
When my son was dying from pancreatic cancer, he was fitted with a morphine pump, that he could adjust himself to dull the immense pain he was enduring.
- His nerves and his brain ascertained the pain level.
- He then adjusted the morphine level.
- He could get very precise control of his pain, because he was measuring it continuously.
But he was only using simple one-term control (proportional).
Derivative Control Can Be Difficult To Get Right And Can Even Go Unstable
Derivative control is mainly to stop overshoot, but sometimes you will find that it can go unstable, so two-term(proportional+integral) controllers will be used.
How I Control My INR
As I said earlier, I am on Warfarin for life and test my INR with a Roche meter.
The NHS typically tests patients about once every six weeks, which in my opinion as a Control Engineer is too infrequent.
I usually test myself a couple of times a week.
But every so often, I evaluate what daily dose gives me an equilibrium INR level of 2.5.
For the last three years, I have found a dose of 3.75 mg keeps me more or less on 2.5.
- As Warfarin comes in 1, 3, 5 and 10 mg. tablets, I alternate 3.5 and 4 mg.
- Warfarin tablets are easily cut in half using a sharp knife.
- I record INR and dose in a spreadsheet.
I have been doing this now for over ten years.
Is This A Unique Property Of Warfarin?
In this time, I have had five medical procedures, where surgeons were worried, that as I was on Warfarin, I might bleed too much.
For the first, which was to remove a lump from my mouth, the private surgeon wanted to charge extra for an anaesthetist. In the end, I asked what INR he wanted and he said 2.1 should be OK!
- So I reduced the Warfarin level and tested every day.
- I judged it correctly and had an INR of 2.1 on the day of the operation.
- The operation went incredibly well and I went home on public transport.
- The lump turned out to be benign.
- I’ve not had another lump.
After the operation, I increased the Warfarin level and tested every day, until it regained a level of 2.5.
On analysing my doses through the date of the operation, I found that the total amount of Warfarin, I didn’t take to reduce my INR to 2.1, was the same as I took to bring it back up again to 2.5.
Is this a unique property of Warfarin?
Since then I’ve had two cataract operations performed in a private hospital, where the NHS paid. Interestingly, they wouldn’t trust my own INR readings, so I had to get my GP to take the measurement.
I’ve also had gallstones removed by endoscopy at the local Homerton NHS hospital.
- For cases like mine, the hospital hire in a surgeon from the posh Wellington private hospital for one day a week, who brings the specialist tools needed.
- I wrote about this in Goodbye To My Gallstones.
- As it was a more serious procedure, I reduced my INR to a requested 1.0.
Interestingly, I still have my gall bladder, but the surgeon put it on notice to behave.
Conclusion
I would totally agree with the conclusion given in the PERSONAL‐CovidBP Trial.
Personalized dose titration with amlodipine was safe, well tolerated, and efficacious in treating primary hypertension. The majority of participants achieved BP control on novel doses, and with personalization of dose there were no trial discontinuations due to drug intolerance. App‐assisted remote clinician dose titration may better balance BP control and adverse effects and help optimize long‐term care.
I would add some conclusions of my own.
- The app used in the PERSONAL‐CovidBP Trial, seems to have had a good algorithm.
- I suspect the app could also be Internet-based.
These are some general conclusions.
- If you are on Warfarin and have access to a Roche meter, it is possible to lower your INR to the value required by a surgeon for an operation or a procedure.
- Since starting to take Warfarin, I have had four operations or procedures, where others would have had anaesthetic or a sedative.
- In those four operations, I was able to go home on public transport. If I still drove a car, I could have driven home afterwards.
- Private hospitals like to use an anesthetist, as it pumps up the bill.
- Avoiding anaesthesia must save hospitals money.
Well designed apps, based on Control Engineering principles, that help the patient take the best dose of a drug will become more common.
Hospital Pioneers Cancer Service For Over 70s That Saves Lives And Money
The title of this post, is the same as that of this article in The Times.
This is the sub-heading.
Treatment is adapted to take into account age-related illnesses, such as heart disease, diabetes and dementia.
These three paragraphs outline, what the Christie Hospital is doing.
The Christie Hospital in Manchester is pioneering a specialist cancer service for elderly patients under plans to tackle a “silver tsunami” of cases.
More than 200 patients have been treated by the new team, which was set up to meet the more complex care needs of an ageing population.
The service has nearly halved the number of unplanned hospital admissions among older cancer patients, improving survival and quality of life.
But it’s the graph that follows that I find interesting.
It shows the cancer incidence rate (per 100,000 population) in 2020 by gender and age at diagnosis.
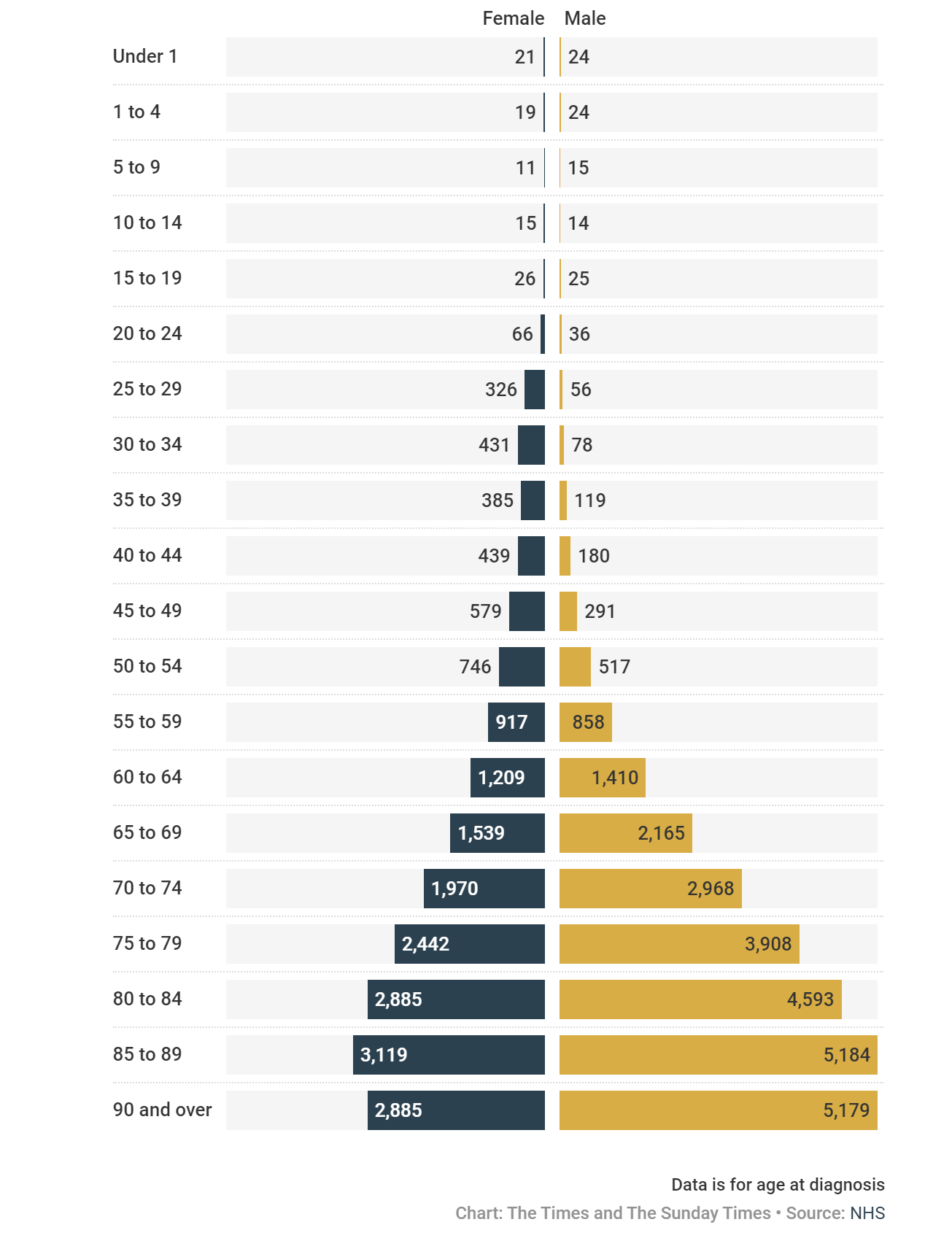
I am a control engineer and statistician and one of the most interesting things in a graph like this is the rate of increase or in this graph’s case the rate of decrease, as the graph effectively has the present at the top.
I have used an old trick and looked at the difference between the groups and the difference between the difference.
Note.
- It seems that the rate of increase of cancer diagnosis with age seems to increase with ages of 60-64 and 25-29.
- This would seem to correspond to those born before 1960 and those born before 1995.
- As a coeliac, I know that the first test for coeliac disease, which used endoscopy was introduced around 1960.
- The modern genetic test for coeliac disease was developed in the 1990s.
Is it coincidence, that the rate of increase of cancer diagnosis with age seems to increase, when a better diagnosis for coeliac disease was introduced?
These are my thoughts!
Coeliac Disease And Me
I am coeliac and I was born in 1947. I wasn’t diagnosed as coeliac until 1997.
I was an unhealthy child, with all sorts of avenues being chased, so in the end they just took my tonsils out.
- It should be remembered, that there was no test for coeliac disease in children until 1960.
- I’ve also only met one coeliac older than me and both her parents were GPs and she was diagnosed by food elimination.
- In fact, I never met a coeliac until I was about 25. He was the two-year-old son of one of C’s friends.
At fifty, an elderly locum gave me a present of a blood test to clear up my long-term health problems. The results showed that my body had very little Vitamin B12. Injections didn’t improve the level, so my GP sent me to Addenbrooke’s.
It was a Monday and all the consultant did was ask a nurse to take several vials of blood. He didn’t ask me any relevant questions or even touch me.
On the Wednesday morning, I got a letter from the hospital saying I was probably coeliac and it would be confirmed by endoscopy.
I must have been one of the first to have been diagnosed by a genetic test on a sample of blood.
Coeliac Disease And My Youngest Son
My youngest son was born in 1972 and after my diagnosis, my late wife felt he was coeliac, as physically he was so like me. But neither him nor our other two sons would get themselves tested.
I am now sure he was coeliac, as his daughter was born with a congenital hernia of the diaphragm and Swedish research says can happen with coeliac fathers. Luckily, she was born in the Royal London Hospital and thanks to heroic surgery at a few days old, she survived and is now in her first year at Southampton University.
Sadly my youngest son died of pancreatic cancer in 2011.
Coeliac Disease And Cancer
Nottingham University have shown that if you are coeliac and stick to a gluten-free diet, you are twenty-five percent less likely to suffer from cancer.
Cancer in the Over Sixties
The following is an extract from A Thought On Deaths Of The Elderly From Covid-19, which I wrote in April 2020.
How many undiagnosed coeliacs are there in those over seventy, who because they are coeliacs, have a compromised immune system?
I would be undiagnosed but for that elderly locum!
How many other coeliacs are there in the UK population?
- Age UK has a figure of twelve million who are over 65 in the UK.
- If 1-in-100, as stated by Coeliac UK, in the UK are coeliac, that is 120,000 coeliacs over 65, who are too old to have been diagnosed as a child, because no test existed.
Note that as of today 177,388 have been diagnosed with Covid-19.
Could the drop in the cancer rate of those born before 1960 be because of the availability of a test for coeliac disease, so that if they were a sickly child like me, they would be diagnosed? As I said earlier diagnosed coeliacs have a lower cancer rate than the general population.
Cancer in the Under Thirties
I was diagnosed in 1997 by a genetic blood test and there is no doubt that I have coeliac disease.
As the test is so simple, I wonder what proportion of coeliacs born since the Millennium have been diagnosed.
And how does this contribute to the drop in cancer cases?
More Research Needs To Be Done
It is obvious to me, that research needs to be done into the link between undiagnosed coeliacs and cancer.
It might be prudent to test every cancer patient for coeliac disease. My GP told me, that the test is not expensive and generally gives the right result.
Bonus For GPs If Patients Join Drug Trials In Plan To Lure Firms To NHS
The title of this post, is the same as that of this article on The Times.
This is the sub-heading.
£650m boost for medical research after number of participants slumps
These three paragraphs outline what is to be done.
Tens of thousands more patients will be signed up for clinical trials as ministers promise drug companies better access to the NHS to expand the economy and develop cutting-edge treatments.
Jeremy Hunt, the chancellor, is promising a £650 million package to boost life sciences as he attempts to lure pharmaceutical giants to Britain.
GPs will be offered financial incentives to recruit patients into trials of new treatments and hospitals will be given research targets under plans to reverse a slump in clinical testing while the NHS struggles with the backlog from Covid-19.
It all sounds good to me.
I have been involved in several trials and medical research projects.
- As part of my coeliac disease diagnosis, one endoscopy was performed by Rebecca Fitzgerald at Cambridge, as she was taking samples of bile fluids for her research into Barrett’s esophagus.
- After the death of my wife, I was interviewed by PhD students in the Psychology Department at Liverpool University for their research into widowhood.
- Oxford University interviewed me on diet for their coeliac disease research.
- After my stroke, I spent an entertaining afternoon at the University of East London doing balance tests by computer. Their aim was to develop a reliable balance test for stroke and other patients, that could be carried out by physiotherapists quickly, than by more expensive doctors.
- I have also been on a drug trial at Queen Mary University, but that drug was useless and had no good or bad affects, so the trial was halted. However, it did lead to other enjoyable activities in the field of patient relations with treatment and research.
As a confirmed coward, I should note that with the exception of the drug trial, all of the other projects were low risk.
I should say, that I also sponsor pancreatic cancer research at Liverpool University, in memory of my son, who died from the disease. I wrote about the first Liverpool project in There’s More To Liverpool Than Football And The Beatles!.
A Database Of Projects Open For Volunteers
I believe that this is needed, so that those like me, who like to contribute to research can volunteer.
Perhaps some of the £650 million, that has been promised by Jeremy Hunt, could be used to create the database.
I also believe the database could be used for other non-medical research.
Possible Coeliacs Should Get Tested
I was diagnosed as a coeliac by both the quick genetic test and the gold standard of endoscopy.
The genetic test is no more painful than any other blood test, but many people are afraid of endoscopy.
I have had four endoscopies.
- Two to check I had coeliac disease.
- One to investigate a problem in my gut with an ultrasound probe, which turned out to be gallstones.
- One to remove the gallstones, by punching a hold in my gut and then inserting and inflating a balloon to force them out.
Only for the last procedure, did I have any form of sedative. I was game, but the surgeon wasn’t!
Note that gallstones are often associated with coeliacs! As are cataracts, which I’ve also had removed from both eyes.
Yesterday in Liverpool, I had chats with two possible coeliacs, one of whom actually had a coeliac mother and the other a gluten-intolerant daughter.
This page on the NHS web site is an overview about Coeliac Disease.
Under Diagnosis Of Coeliac Disease, this is said.
First-degree relatives of people with coeliac disease should be tested.
My three sons didn’t get tested, despite both my late wife and myself insisting after my diagnosis.
Conclusion
If it’s ever suggested you be tested for coeliac disease, you should get tested.
It’s not a big deal these days.
Coeliac Journey Through Covid-19 – Medical Research
Medical Research
I first got involved as a lab-rat in medical research, when I had my second endoscopy to check for coeliac disease at Addenbrooke’s Hospital in 1997. Rebecca Fitzgerald took a sample of fluid from my gut for her Barrett’s oesophagus research.
After my wife died, I asked my contact in Alumni Relations at Liverpool University, if they did widowhood research.
They are one of the few universities that do and I did several interviews for PhD students in the unit, which is in the Psychology Department. It was very much a positive experience and certainly helped with my grieving.
In some ways the most enjoyable piece of research I have been involved in, was at the University of East London, where they were using computers to measure the balance of those recovering from strokes.
My GP also suggested that I get involved in drug tests at Queen Mary University. The tests were abandoned as the drug didn’t have any good or bad effects, but now I’m one of the William Harvey Centre’s lab-rats.
I also help to sponsor pancreatic cancer research at Liverpool University in memory of my son.
In There’s More To Liverpool Than Football And The Beatles!, I detail some research, that I sponsored in a small way.
I may be tempted to do the fund-raising trip again.
I always advise people to get involved in medical or psychological research, as I have found it such a beneficial experience.
One thing that is needed, is an on-line database of all research projects that are looking for volunteers.
Remember, that much medical and psychological research is about as dangerous as meeting someone in a GP’s surgery for a chat or perhaps in a cafe and having a coffee.
Coeliac Journey Through Covid-19 – Coeliac Diagnosis
Coeliac Diagnosis
My health was very variable as a child.
I would often have months off school and my health only really improved, when my parents bought a second home in Felixstowe, where we spent most of our holidays.
Perhaps it was the sea air, as going to Liverpool University didn’t seem to adversely affect my health.
I had been having gut problems for years and then in Autumn 1997, I didn’t see my GP, but a very elderly locum, who as I had recently had my fiftieth birthday, gave me a present of my first blood test.
It turned out that I was very low on B12 and a course of B12 injections was arranged.
As the injections didn’t raise my levels, an appointment was made to see a consultant at Addenbrooke’s Hospital in Cambridge.
It was a Monday, when I went to the appointment and after a quick chat and no examination, the consultant said that they would take some blood. Which they did!
Within forty-eight hours a letter arrived on my door-mat saying that I was probably coeliac and it would be confirmed by endoscopy.
Two endoscopies without sedative or anaesthetic were performed and I was confirmed as coeliac.
The first was performed by Dr. Richard Hardwick and the second by Dr. Rebecca Fitzgerald.
My gut health has been better since, I’ve been on a gluten-free diet, backed up by three-monthly B12 injections.
A few years later, I was talking to a gastroenterologist in Cambridge and he told me that he thought he had more coeliac patients than any other in England.
The manager of Carluccio’s in the city, also told me that they sold a very high percentage of gluten-free food.
Were Cambridge testing a genetic test for coeliac disease or was it just a Whack-A-Coeliac policy?
They certainly had everything geared up for high-speed diagnosis. They even did the endoscopies without a sedative, so they didn’t need any recovery beds.
High Risk Of Coeliac Disease In Punjabis. Epidemiological Study In The South Asian And European Populations Of Leicestershire
The title of this post, is the same as that of this peer-reviewed paper on PubMed.gov.
This is the abstract of the paper.
The purpose of this study was to measure the incidence of coeliac disease in different ethnic communities and investigate the hypothesis that the incidence is decreasing in most European countries and the role incomplete retrieval of data may play. In a retrospective study of histologically confirmed cases of coeliac disease between 1975 and 1989 in the City of Leicester, 106 patients with coeliac disease were identified. Of these 86 were European and 20 Asian. The overall incidence of coeliac disease in Europeans was 2.5/10(5)/year (95% CI 2-3.2), in Gujaratis 0.9/10(5)/year (95% CI 0.4-1.8), and in Punjabis 6.9 (95% CI 3.2-12.3). These differences were independent of religious belief. The relative risk to Punjabis compared with Europeans is 2.9 (95% CI 1.5-5.3; chi 2 = 12.5, p < 0.01) and to Gujaratis 8.1 (95% CI 3-22.4; chi 2 = 25; p < 0.001). Gujaratis were at 0.4 risk of Europeans (90% CI 0.2-0.8; chi 2 = 6.7; p < 0.01). The incidence in the urban populations of Leicester was 6/10(5)/year (95% CI 1.3-1.9) which was significantly lower than the 3.2/10(5)/year (95% CI 2.7-3.8; chi 2 = 5.6; p < 0.001) in surrounding rural areas. This study shows that the incidence of coeliac disease in Punjabis (Sikhs, Hindus and Muslims) is 8 times higher than in Gujaratis (Hindus and Muslims) and 4 times higher than in Europeans in Leicester.
I find the last sentence in particular very significant.
I’m no medic, but I think it is reasonable to assume, that in a particular community for every diagnosed coeliac, there will be several undiagnosed coeliacs out there.
In this overview of coeliac disease on the NHS web site, this is said about the incidence of coeliac disease.
Coeliac disease is a condition that affects at least 1 in every 100 people in the UK.
But some experts think this may be underestimated because milder cases may go undiagnosed or be misdiagnosed as other digestive conditions, such as irritable bowel syndrome (IBS).
Reported cases of coeliac disease are around 3 times higher in women than men.
The one-in-100 figure is often used in web pages in European countries or Australia, Canada and the United States, so I’ll go along with that.
So does that mean that Punjabis living in Leicester, have a one-in-twenty-five likelihood of being coeliac?
Whether you have been diagnosed though, is a matter of pure luck.
I had been having gut problems for years and then one Autumn, I didn’t see my GP, but a very elderly locum, who as I had recently had my fiftieth birthday, gave me a present of my first blood test.
It turned out my B12 levels were very low and after several months of B12 injections, which made little difference to my B12, my GP decided to send me to a consultant at Addenbrooke’s Hospital in Cambridge.
My appointment was on a Monday morning and consultant took about ten minutes to ask a few questions, after which he said they would take a few bloods.
On the Wednesday morning, I received a letter that said, that I was probably suffering from coeliac disease and this would be confirmed by endoscopy.
Was I diagnosed solely by analysis of my blood? This was in 1997, which is after the date of the Leicester study.
Two endoscopies without sedative or anaesthetic were performed and I was confirmed as coeliac.
The first was performed by Dr. Richard Hardwick and the second by Dr. Rebecca Fitzgerald.
Both doctors feature in this story on the Cambridge University Hospitals web site, which is entitled Familial Gastric Cancer – Case Study.
My problems have been minor compared to the two sisters in the story.
My luck had been good and I recommend that everyone who feels they could be coeliac should get themselves tested.
Cases Of Covid-19 In Leicestershire
This article on the Leicester Mercury is entitled 11 Areas Of Leicestershire Have Among Worst Infection Rates in the UK.
In Coeliac Disease: Can We Avert The Impending Epidemic In India?, I started like this.
The title of this post, is the same as that of this article on the Indian Journal Of Research Medicine.
With the high levels of COVID-19 in Leicester and an Indian population who make up 28.3 % of the population of the city, I was searching the internet to see if there was any connection between those of Indian heritage and coeliac disease.
I know you should not try to prove a theory. But as a coeliac, I’m very interested to see how the millions of diagnosed coeliacs on a gluten-free diet like me, are faring in this pandemic.
I then talk about some extracts from the Indian research.
In a section entitled, which is entitled All Wheats Are Not Equal, I say this.
The other dimension to this problem is that not all wheat is alike when it comes to inducing celiac disease. The ancient or diploid wheats (e.g. Triticum monococcum) are poorly antigenic, while the modern hexaploid wheats e.g. Triticum aestivum) have highly antigenic glutens, more capable of inducing celiac disease in India, for centuries, grew diploid and later tetraploid wheat which is less antigenic, while hexaploid wheat used in making bread is recently introduced. Thus a change back to older varieties of wheat may have public health consequences.
So did all these factors come together to create the high levels of Covid-19 in Leicestershire?
Conclusion
I am getting bored with saying this. More research needs to be done!
