Glasgow Bin Lorry Driver Should Have Been Charged
According to this article on the BBC web site, a former prosecutor has said that the driver of the Glasgow bin lorry, that killed six people should have been charged. The report starts like this.
A former senior prosecutor has strongly criticised the decision not to charge the driver at the centre of the Glasgow bin lorry tragedy.
Brian McConachie QC said there was sufficient evidence to prosecute Harry Clarke.
He said the Crown Office had “jumped the gun” in not pressing charges.
I feel very strongly about this. After I had my stroke, my eyesight was terrible and I decided that to start driving again would not be a responsible thing to do.
My current GP, who has seen me for three years, feels that if I wanted to, I could get my licence back.
But quite frankly I couldn’t be bothered. And I have a lot of backing from my healthy bank account.
What worries me, is how many other Harry Clarkes are there driving around?
In the last four years, I had lifts from other drivers a few times and quite frankly with two of them my eyesight seemed better.
My eyesight problem incidentally, is that I can’t see moving objects low down on the left. So one nightmare on the street, is meeting a crocodile of young children, say being led by their teachers. Luckily I haven’t done anything I shouldn’t! A few times though, people wheeling cases have pulled in front of me from the left and I’ve bumped into the case. Only once have I ended up on the ground, as usually my balancing skills which are still tip-top have got me out of trouble.
Harry Clarke was extremely irresponsible, in not reporting his failing health problems!
Incidentally, if say I was fifty and had got my eyesight problem, as I live in London, I would get a Freedom Pass, entitling me to free public transport in Greater London. I get one anyway as I’m over the qualifying age.
Dementia Has Stabilised
According to this report on the BBC web site, research from the University of Cambridge has shown that dementia levels are stabilising.
A few years ago, Oxford University proved a link between having low B12 levels at 50 and dementia, if you had dementia in your family.
Could it be, that GPs, who now check out bloods regularly are having an effect?
When first tested at 50, my B12 levels were non-existent. Now at 68, they’re spot on!
And what is one way to help your B12 levels? – Go gluten free!
As other studies at other world-class universities, like Nottingham, have shown that a gluten-free lifestyle lowers your changes of getting cancer, I think that going gluten-free because of my coeliac disease, wasn’t one of the worst lifestyle decisions I made.
INR Testing Around A Simple Procedure
A couple of weeks ago, my dentist found a small lump in my mouth,so he advised getting it removed and tested to see that it was nothing serious. The procedure was booked to take place on Thursday, the 30th of July and he advised me to make sure my INR was lower than 2.4 and not to take any Warfarin on the day before. Obviously, he didn’t want me to bleed too much, especially as the position of the lump made stitching impossible.
My INR had been 2.6, 2.5 and 2.6 on the Sunday, Monday and Tuesday, taking my normal dose of 4 mg., which as I take it most days, is unsurprisingly my average dose.
On the Tuesday, to lower te INR slightly, I cut my dose to just 1 mg., with the consequence by Wednesday morning the INR had dropped to 2.3. As the doctor had said no Warfarin on the Wednesday, my Control Engineering training said that could drop the INR below 2. So I just took 1 and the INR was 2.1 on the day f the operation.
After the operation, as I wasn’t bleeding I took 3 mg of Warfarin, but by the Friday morning my INR had dropped to 1.6, so that evening I took 6 mg. On the Saturday morning, the INR had gone up a bit to 1.7, so to nudge it towards the desired value of 2.5, I took six that day.
In the week of the operation despite changing the dose to control my INR, I sactually averaged 3.8 mg. over the week.
Since then I’ve taken my normal 4 mg. and my INR has been fairly steady around 2.4.
I think this exercise shows the value of self-testing your INR. Admittedly, I was employing my Control Engineering training and experience to give the doctor what he wanted and keep my INR at a reasonably safe level, but the ability to self-test regularly around an operation must make things better for everybody concerned.
The doctor told me afterwards that I hadn’t bled too much, but then when I’m cut by a professional as opposed to torn in a fall say, I don’t seem to bleed much!
In the end, the lump had been removed and I heard today, that it was totally benign.
Do We Have Too Many Breast Cancer Charities?
That may be a controversial thing to say, but these posters for a new breast cancer charity have been appearing everywhere in London.

Do We Have Too Many Breast Cancer Charities?
Now C successfully survived breast cancer, so it is not a subject I know nothing about.
But I think now, that some of the most promising cancer research, like looking at the genetics, is very expensive and covers the whole spectrum of cancers.
So surely, this is where we should give our money. I incidentally subscribe to three different cancer charities, none of which are directly linked to breast cancer.
Although, Cancer Research UK, which I support, does support research into breast cancer.
Hope For Sufferers Of Cystic Fibrosis?
This morning, the BBC is showing this report entitled Gene therapy stabilises lungs of cystic fibrosis patients.
It is encouraging news, but also I suspect that it is very interesting technologically.
The genes are actually give to the patient through an inhaler, in a much simpler treatment regime.
Could Britain Become The World’s Health Hub?
Matt Ridley in The Times yesterday has an article entitled Britain has the chance to be the world’s doctor. This is an extract.
A new report commissioned by three parliamentarians, Meg Hillier, MP, Lord Crisp (former chief executive of the NHS) and the surgeon Lord Kakkar, and written by researchers at the London School of Hygiene and Tropical Medicine, makes the case that Britain is well placed to become the world’s “health hub”. Just as the City of London is the world’s financial centre and Wimbledon is the centre of tennis, so Britain is already a surprisingly dominant player in research, practice, policy and regulation when it comes to health, and widely emulated around the world. There is an opportunity here.
I have been privileged in my life and have had insight in London, Cambridge and Liverpool into substantial developments and research that are going to make the world a healthier place.
It is our pre-eminence in health research and the related fields like information, that is driving the world’s health forwards.
Ridley gives some surprising facts, like that even the much-criticised NICE has an international offshoot that gives advice to countries with limited health funding.
It is an article that gives a positive outlook on the future and finishes with this statement.
If America is the world’s soldier, Germany its engineer, Brazil its farmer, China its manufacturer and India its service provider, then Britain can be the world’s doctor.
Everybody worried about the future of healthcare, should read this article.
Do We Featherbed Groups In Society?
I got my monthly State Pension today and at £677.16, that will do me for my day-to-day expenses for the next month. It doesn’t cover trips out of London, but it does allow me the odd light lunch in a restaurant.
But I also get other benefits just because of my circumstances, as a 67-year-old man, who lives alone.
I get a Council Tax discount because I live alone. But is that right as I live in a family house with a garage in a desirable part of London? If I didn’t get it, I’d still live here as that would be my choice, but I am blocking someone more worthy than me of buying this house.
I have a highly-insulated house with an efficient boiler, but should I get a winter fuel allowance? It would be better if the money was not paid at all, but used to improve our housing stock’s energy efficiency, so that those on a pension actually saved the money all through the year.
I have a Freedom Pass, which gives me free transport on buses, Underground, Overground and trains within the Central London area. This is one of the reasons I moved to Dalston. But is it too generous on the one hand and not universal enough on the other? Surely, a better system, would be one where you nominated your bank card as your transport pass and in the free areas, the system didn’t charge you. The advantage of this would be that London could enter into reciprocal arrangements with areas like Birmingham, Liverpool, Manchester and Newcastle, so that we could use each other’s concessionary area at a discount. Would this encourage more of us to travel to explore the country and perhaps spend money in attractions, cafes and shops, we wouldn’t dream of visiting now?
This morning according to this report on the BBC, the Liberal Democrats are saying that those who have a second house they use in a beautiful area, should pay double Council Tax on their second home. Here! Here!
I live in Central London and I am starting to resent the traffic. Not because I drive, but because of the pollution and noise often put out by cars used as glorified shopping trolleys and baby buggies. We let all drivers get off too lightly with the problems they cause in cities and if they got the message, we may see more cycling and walking, and better air quality. We might even see better delivery systems for goods, where transmissions were hybrid or electric, like London’s newer buses.
It will happen eventually, that all cars pay road charges based on mileage, fuel used and congestion. But I doubt we’ll see it soon, as there are no votes in it. It’ll probably be introduced in London first, as cycling gets more common and Crossrail shows everybody what real railways can be like.
But would a city like Birmingham, where the car is king, and pedestrians are targets to hit when crossing the road, accept charging to pay for the updating of the numerous railways and more trams in the city?
And then there’s lifestyle, fitness and health!
Many people drink, eat and smoke too much and governments don’t really discourage it forcefully. It would be an interesting exercise for a town or city to declare a city centre non-smoking and see what happens. I can remember, when ahead of the smoking ban the landlord of my local pub in Suffolk declared it a smoke-free zone. He got some moans, but not from his bank manager.
The NHS is in crisis, but this is mainly a problem of the irresponsible patients making. So if we can get people back to the straight and narrow, we might help the dear old NHS out.
For a start, I would like to see a law, that no-one could stand for elected office or sit on the board of an NHS body, if they were a smoker!
I could go on a lot more. But we must all change our lifestyle, if we want this country to be a place, that is really worth living in.
Hospital Closure Protests
Yesterday’s BBC London local news led with a story about how the hospitals of Epsom and St. Helier NHS Trust will be redeveloped.
They currently have three hospitals at Epsom, St. Helier and Sutton and consultants overhead on a train, are saying that a new hospital will be developed on one of the sites.
From what the report said, the locals want to keep all hospitals, which may not be the most economic or practical solutions.
I have looked at Google Earth images and the details on how you get to these hospitals and I suspect that the only practical way to get to these hospitals is by car or taxi. But as they probably charge an arm and a leg for parking, this is probably something that gets protested about all the time.
If they do build a new hospital it must be easily accessible by public transport. At present all sites need a long walk to all except Epsom, which is obviously a policy designed to discourage poorly and elderly patients and visitors without their own transport. There have been plans to link St. Helier hospital on the Tramlink, but nothing seems to be happening in that area. This is the Google Earth image for the hospital.
St. Helier Hospital
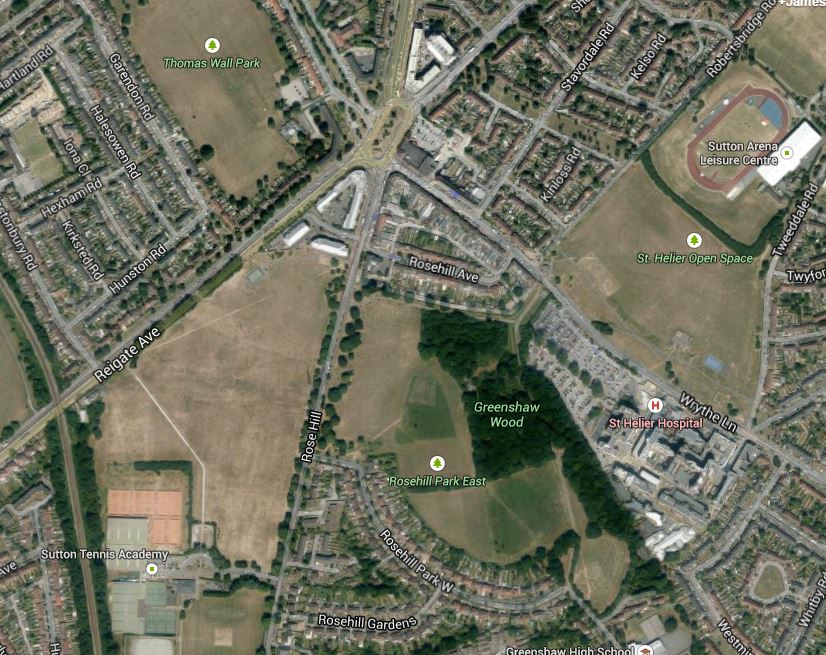
Surely, if you are going to create a new super-hospital it must have first-class public transport links. This article in the Local Guardian shows the route of the proposed Tramlink extension.
St. Helier Tramlink
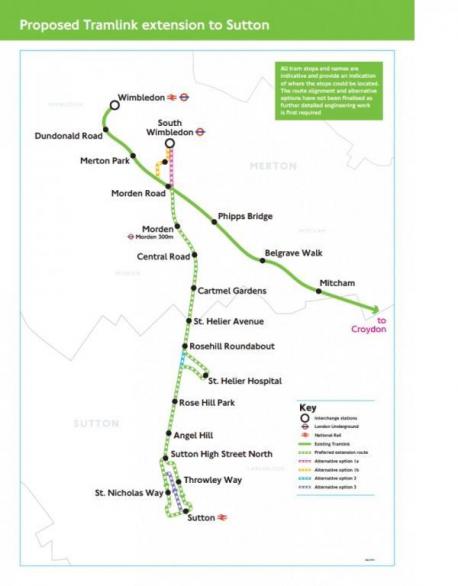
I would assume that the loop to St. Helier Hospital includes street running or goes through Rose Hill Park. This a Google Earth image of the area.

St. Helier Tramlink Detail
The roundabout at the top left is Rosehill roundabout, which is planned to have a tram stop and the hospital is at the bottom right.
It would seem feasible to run the Tramlink to the hospital, but would the street running and/or possible loss of green space, create a lot of opposition?
A survey on the Merton Council web site is very supportive of Tramlink going to the hospital.
An interesting fact is that there is a frequent train service, that takes just ten minutes between Epsom and Sutton stations, so if a super-hospital was built on the St. Helier site, getting there from Epsom wouldn’t be difficult, provided of course the Tramlink extension was built.
If we look at Epsom Hospital becoming the super-hospital, then here is a Google Earth image that shows both Epsom station and the hospital.

Epsom Station And Hospital
The station is at the top and the hospital is indicated by the red arrow at the bottom.
From experience of the area years ago, it is not an easy walk and should a super-hospital be served by buses alone?
The other site is to build it on the old Sutton Hospital. But this is only served by buses from Sutton station, as is the nearby world-class Royal Marsden Hospital. This Google Earth image shows the two hospitals and the nearest rail station at Belmont.

Sutton Hospitals And Belmont Station
There could be possibilities to sort out the transport links in some way to Belmont station, but it only has an infrequent service with nothing on a Sunday.
I have a feeling that if the Tramlink extension is built between Wimbledon and Sutton stations, that if tram-trains were used they could extend down the Epsom Downs branch, with perhaps a loop to serve the developing Health Campus based on the Royal Marsden and perhaps a super-hospital built at Sutton.
Avoiding The Real Issues In The NHS
All the political parties seem to be promising more and more to the NHS in this election, be it money, drugs, doctors, nurses or midwives.
Money could be the least of the problems, as it will probably come from improvements to the economy or some tax-the-rich measure, depending on your political point of view.
As drugs are not really a drug problem, but usually a money one, we are left with where to we get the tens of thousands of staff we need to provide health-care.
The trouble is that being a health professional, is a skill you can use anywhere in the world, as all human beings are the same under the skin, even if they come in various colours, speak different languages and have certain different diseases governed by genetics or environment. So just as we can recruit paramedics from the Antipodes, nurses from the Philippines and doctors from virtually everywhere, other countries can entice our health professionals away.
We live in an increasingly global society, and working abroad for a few years is often in many peoples desired career profile, be it in health care or not. Healthcare like certain other professions is one of those that gives you a passport to a lot of interesting places.
All manpower planning in the NHS seems to believe that those trained here, will stay here. But all good training does is hand everybody that passport to travel.
To make matters worse, good training for some professions, is an excellent grounding to starting a business or working in the private sector.
So the first issue we must face, is this one of where do we get the staff. The NHS has shown itself to be not very innovative in this area.
Some have suggested in the past, that anybody trained in the NHS must contract to work for the service for so many years. This is just cloud-cuckoo thinking.
The one positive thing that can be done to help staff is to provide better working conditions and rewards for those working in the NHS. Most of the NHS buildings, I’ve seen in the last ten years have been pretty sound, with perhaps the odd exception, so we must look at the problems of staff with respect to organisation, management, pay and pensions.
What I do find interesting is that all of the Practice Nurses I’ve met in GPs surgeries seem to be so much happier in their work than those in hospitals. It’s only a small survey, but it does say something about the difference between GP’s surgeries and hospitals.
When I’ve spent time in hospital in the past few years, it has been been twice in good NHS hospitals and once in an expensive private one in Hong Kong. There was little difference in the equipment or methods used, but as an IT professional of some years experience, I don’t believe that hospital systems are what an engineer or manager would accept if they worked in say a modern car factory in the UK.
So we must get hospital and GP health systems to the levels that patients and staff expect in their personal life.
Where is an on-line copy of my health record, that I can read to get to the bottom of my problems, that seem to occur seasonally in the Spring?
But things are changing and we must create a health communication and information system, that is an order of magnitude better than what we have today.
No political party is saying they’ll fix this important gap in the NHS.
Everything in our lives is going on to our computers or phones, but healthcare in the NHS hasn’t changed that much since I was born in 1947.
Some people rightly worry about such a computer system. But at its best it would only be like an on-line shopping system, where if you don’t see what you need on-line at your favourite store, you go and look at a physical one.
In all the politicians posturing on health, they very much ignore the users of the NHS and what they can do to improve the service and its efficiency.
I would be interested to see an analysis of how much the average patient costs the NHS. I suspect that because of the lack of a fully joined-up computer system, if I had complete access and wanted to find out how much I cost the NHS last year, no accurate value could be calculated.
Many people calculate their motoring costs to the last penny, but even if they wanted to, it’s probably impossible with healthcare, even though all the data is there.
Eventually, everybody will have this figure, as it could be a powerful tool for a GP to classify and better treat their patients and as a motivator to patients to improve their lifestyle. You’ll never change some patients, but many could be nudged in the right direction.
We must also do more to ease our load on the NHS. On a personal level, I look after my INR, by doing my own tests. A Committee of MPs has stated that all NHS patients who can, should do their own testing to save the NHS a lot of money.
How many other measurements can be taken by patients to ease the load? And are we doing enough to encourage more and better devices?
In no political party’s pontifications on the NHS, can I find anything about bringing the patient more into his or her own healthcare. But many doctors and nurses have said to me that we should take more responsibility for our own health.
After all, many of us now carry a tablet or phone, that has more computing and information accessing capability than existed anywhere ten years ago. Is this being used to give us better healthcare? Not really!
Political parties are not tackling the problems caused by our poor diet, lifestyle and environment.
Where I live, there are more unhealthy takeaways than you need to try a new one every week of the year. Not one sells any gluten-free food, so their chances of seducing me with their crap is non-existent.
Even the Sainsburys Local that I use is not a store,where you can always get the staples you need to create a healthy meal. Yesterday, I needed a couple of haddock fillets for supper, but except for some very bedraggled and unappetising cod, there was no uncoated fish. So I had to take a bus to the Angel to get some from Waitrose. Does a lack of healthy food locally mean that many don’t eat as healthily as I do? I am out and about in London most days using my Freedom Pass, so it is not difficult for me to pick up what I need on the go. But a young mother with an infant in a buggy doesn’t have that luxury. It’s not the shops’ fault, as they only stock what the shop sells!
The only positive thing government can do in this area, is to give local authorities more power to decide what shops they allow in their area.
I haven’t seen anything like this in any manifesto.
We should also do things to curb air pollution, which can get bad at times. All city centre transport, should either be electric or very low emission vehicles.
But again, no-one wants to annoy people, except the Greens, who won’t win anyway.
I suppose smoking comes into this area. Any candidate for London Mayor, who decides to ban it in public parks, squares and in the vicinity of bus stops gets my vote next time.
Perhaps candidates for the election, should have to declare if they smoke or not and what car they drive on the ballot paper!
Do we also give our children an education that will help them get through the minefield that is health? We give sex education in schools, but surely health education is just as, if not more important!
We need to think radically, about how we deliver healthcare and before we throw money at it, we should sort out the details on how it is delivered, how it interacts with patients and the fasctors that affect it.
Conservative 1940s thinking has failed and we must bring the NHS into the twenty-first century.
The World-Changing Invention Of The Decade
I heard about Stablepharma on the BBC 5 Live Science program.
The delivery of vaccines to isolated places all over the world is very worthwhile and extremely expensive because it needs a lot of refrigeration for the journey.
But read about the technology being developed by Stablepharma.
If this can be made to work, healthcare will never be the same again!
