Gluten Sensitivity And Epilepsy: A Systematic Review
Yesterday, The Times published this article, which was entitled ‘Game-Changing’ NHS Laser Therapy To Prevent Epileptic Seizures.
One reader had made this comment.
Be ace too if they can tweak to help migraine.
I used to suffer from something like migraine about thirty years ago. But after being found to be coeliac and going gluten-free, what ever it was seemed to disappear from my life.
Type “Coeliac Disease and Migraine” into Dr. Google and there are lots of references.
This indicates to me that serious scientists and doctors, must believe there could be a link.
There certainly is with me and going gluten-free eased my migraine-like symptoms.
I then typed “Coeliac Disease and Epilepsy” into Dr. Google and found this paper, which was entitled Gluten Sensitivity And Epilepsy: A Systematic Review.
This information is from the Abstract of the paper
Objective
The aim of this systematic review was to establish the prevalence of epilepsy in patients with coeliac disease (CD) or gluten sensitivity (GS) and vice versa and to characterise the phenomenology of the epileptic syndromes that these patients present with.
Methodology
A systematic computer-based literature search was conducted on the PubMed database. Information regarding prevalence, demographics and epilepsy phenomenology was extracted.
Results
Epilepsy is 1.8 times more prevalent in patients with CD, compared to the general population. CD is over 2 times more prevalent in patients with epilepsy compared to the general population. Further studies are necessary to assess the prevalence of GS in epilepsy. The data indicate that the prevalence of CD or GS is higher amongst particular epileptic presentations including in childhood partial epilepsy with occipital paroxysms, in adult patients with fixation off sensitivity (FOS) and in those with temporal lobe epilepsy (TLE) with hippocampal sclerosis. A particularly interesting presentation of epilepsy in the context of gluten-related disorders is a syndrome of coeliac disease, epilepsy and cerebral calcification (CEC syndrome) which is frequently described in the literature. Gluten-free diet (GFD) is effective in the management of epilepsy in 53% of cases, either reducing seizure frequency, enabling reduced doses of antiepileptic drugs or even stopping antiepileptic drugs.
Conclusion
Patients with epilepsy of unknown aetiology should be investigated for serological markers of gluten sensitivity as such patients may benefit from a GFD.
My Thoughts
These are my thoughts.
Coeliacs Prior To 1960
Consider.
- Even if my excellent GP; Doctor Egerton White, felt I was coeliac, there was no test until 1960 for coeliac disease.
- And the test that was developed using endoscopy wasn’t anywhere near to the endoscopies of the present day.
- My late wife, who was a family barrister, likened the test to child abuse on a young child.
- I have heard some terrible horror stories of doctors looking for coeliac disease in young children in the 1950s.
- But there were some successes. A friend of mine, who is in her eighties, was successfully diagnosed by her parents using food elimination. But they were both GPs.
- Recently, I’ve met two elderly ladies, who only in the last couple of years have been diagnosed as coeliacs.
Luckily, I was never tested until 1997 and I was diagnosed in 48 hours, by gene testing.
Methodology
The methodology was based on a systematic computer-based literature search of the PubMed database.
This has these advantages.
- The rules for the search can be published and peer-reviewed.
- Its Wikipedia entry says PubMed is a free database including primarily the MEDLINE database of references and abstracts on life sciences and biomedical topics.
- The technique can surely be applied repeatedly, to see how results are changing with time.
- The search can be modified to analyse any topic, drug or condition, that appears in the PubMed database.
- The analysis could surely be applied to other databases.
As a writer of data analysis software, developing this sort of software, would be really enjoyable.
AstraZeneca Withdraws Covid Vaccine After Drop In Demand
The title of this post, is the same as that of this article on The Times.
This is the first paragraph.
AstraZeneca is withdrawing its Covid-19 vaccine worldwide, citing a “surplus of available updated vaccines” since the pandemic that target newer variants of the virus.
This was my experience of the vaccine.
I am coeliac and have a very strong immune system, as it gets all the fuel it needs.
When I had my first AZ vaccine, my immune system started to attack the chimpanzee adenovirus-based viral vector vaccine.
I felt dreadful and I’ve now been advised by doctors, not to have any more viral vector vaccines.
Interestingly, I had no reaction to the second dose, so my immune system had probably decided it was a friend.
When I had that second dose, there was all the controversy raging, about whether the AZ vaccine causes blood clots.
So I did an experiment, which I described in My INR Readings Before And After My Second AstraZeneca Jab.
I found that my INT bounced all over place, just as when a wheel hits a pothole.
Conclusion
I shall not be taking the AstraZeneca Vaccine for COVID-19 again and would think twice before allowing myself to be injected with a viral vector vaccine.
Study Highlights Increased Risk Of Second Cancers Among Breast Cancer Survivors
The title of this post, is the same as that of this news story from the Cambridge University.
This is the sub-heading.
Survivors of breast cancer are at significantly higher risk of developing second cancers, including endometrial and ovarian cancer for women and prostate cancer for men, according to new research studying data from almost 600,000 patients in England.
These are the first three paragraphs of the story.
For the first time, the research has shown that this risk is higher in people living in areas of greater socioeconomic deprivation.
Breast cancer is the most commonly diagnosed cancer in the UK. Around 56,000 people in the UK are diagnosed each year, the vast majority (over 99%) of whom are women. Improvements in earlier diagnosis and in treatments mean that five year survival rates have been increasing over time, reaching 87% by 2017 in England.
People who survive breast cancer are at risk of second primary cancer, but until now the exact risk has been unclear. Previously published research suggested that women and men who survive breast cancer are at a 24% and 27% greater risk of a non-breast second primary cancer than the wider population respectively. There have been also suggestions that second primary cancer risks differ by the age at breast cancer diagnosis.
I have a few thoughts.
The Data
The story says this about the data.
To provide more accurate estimates, a team led by researchers at the University of Cambridge analysed data from over 580,000 female and over 3,500 male breast cancer survivors diagnosed between 1995 and 2019 using the National Cancer Registration Dataset. The results of their analysis are published today in Lancet Regional Health – Europe.
A large number of cases were analysed and with these types of analysis, more is definitely better.
I would hope that this study will be repeated in a few years, when more data is available.
The Death Of My Wife
This happened to my late wife.
At about 55 in 2004, my wife developed breast cancer. Strangely, it was in the same position, where a car air-bag had bruised her breast, when it went off in an accident, a few years before.
Chemotherapy was recommended and she tried one round at home, but she couldn’t get on with it.
So she eventually had a long course of radiotherapy in Harley Street going up every day on the train. She was also doing as many court cases as she could to pay for it all.
It appeared everything had worked well and in the Autumn of 2007, she was given the all clear for the breast cancer.
But in October 2007, she was diagnosed with a squamous cell carcinoma of the heart.
She died in December 2007 at just 59.
My wife’s second cancer and her death seems to fit the pattern of the patients in the news story.
My Wife’s Genetic Background
This is rather bare, as she was adopted. Although, I do have her plaits from, when the cut them off at 18, as she’d kept them and I found them after she died.
But she didn’t come from a deprived background.
I Am Coeliac
If I have one regret, it’s that I didn’t encourage her to go gluten-free after the first cancer.
It might have boosted her immune system to help.
Conclusion
Anybody, who has breast cancer must beware a second attack of cancer.
Uf it can kill my fit 59-year-old wife, it can kill anyone.
Did A Day In A Class 350 Train Lower My INR?
Yesterday, I went to Birmingham to take pictures of the rebuilt Birmingham University station.
- I travelled by West Midlands Trains catching the 11:23 to Birmingham New Street station, where it arrived at 13:45.
- Coming home, I caught the 15:36 from Birmingham New Street station, which arrived in Euston at 17:49.
So I spent nearly four and a half hours in the train.
This morning, when I measured my INR, it was only 1.8.
Did the weather and the train’s air-conditioning conspire to lower my INR by removing water from my body?
A Redbrick Station For A Redbrick University
My late wife; C and myself, met at Liverpool University in the 1960s.
Liverpool considers itself as the Original Redbrick on its web site.
This Google 3D visualisation shows why.

Note.
- This 3D picture was taken from the East.
- The white building in the bottom-right corner is the Electrical Engineering and Electronics, where I did most of my studying.
- The building above it is the Harold Cohen Library.
- The clock tower in front is part of the Victoria Building.
There’s a lot of redbrick on the University site.
These pictures show University (Birmingham) station.
























Note.
The Architects didn’t spare the red bricks.
- The station has an NHS Clinic
- The bridge has lifts and steps.
- There is a lot of glass.
There are a pair of bi-sexual toilets, which seems to the standard for new stations these days.
Will Other Universities Want A Station?
Here are a few thoughts.
Liverpool University
I wrote about the possibility in A Railway Station At Liverpool University.
This is an extract.
In Liverpool’s Forgotten Tunnel, I showed this map, which shows a proposed reopening of the Wapping Tunnel as a passenger route between Liverpool Central and Edge Hill stations.
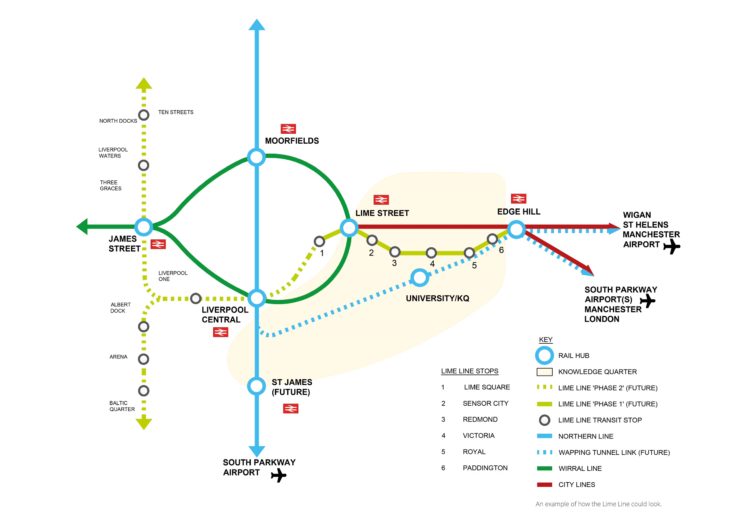
Note.
- The map shows a station at University
- The Wapping Tunnel is shown as a dotted blue line.
- Between four and eight trains per hour (tph) would be running through University station.
Liverpool has other projects on its mind at present, but I wouldn’t rule it out in the future.
Manchester University
This Google Map shows the location of Manchester University.

Note.
- The red arrow picks out a notable building in the University.
- Manchester Piccadilly station is in the North-East corner of the map.
- Manchester Oxford Road station is in the South-West corner of the map.
- In recent years I’ve walked between the two stations.
- The Castlefield Corridor passes through the University.
A station on the Castlefield Corridor could be a possibility.
I Was Kathleened At The Weekend
Saturday
At 0200 on Saturday morning, I couldn’t sleep.
So in the end, I got up, made myself a mug of tea and did Saturday’s puzzles in The Times.
I had no trouble doing them, so my brain function was normal.
But my left hand wasn’t working that well.
I had breakfast in Leon and had a bit of trouble with their sauce containers, but otherwise I was fine.
I did a bit of shopping in M & S on Moorgate and came home.
I wasn’t having any problems.
For the rest of the day, I watched television and listened to the radio.
Sunday
I got up late, as I was probably catching up the sleep from the night before.
I had lunch in Gordon Ramsey’s Street Burger about one.
My left hand wasn’t working that well and I was making a bit of a mess.
After, I got home, I watched television and listened to the radio.
Monday
I slept in late, but as my left hand wasn’t being very co-operative, I had a small bit of trouble dressing, due to an uncooperative left hand.
My INR was 2.0, so I took 5 mg. of Warfarin.
I had breakfast in Leon, where I made a mess with the sauce container.
I then went looking for a book, which I couldn’t find.
Tuesday
Everything seems better today.
My INR was 2.1, so I took 5 mg. of Warfarin.
I did my usual Monday morning trip, of visit to Marks & Spencer for about three days of food and then had breakfast in Leon.
Conclusion
This seems to be a pattern.
- A storm goes through, I can’t sleep and after some drinks of tea or zero alcohol beer, I feel a bit better.
- My left hand often stops co-operating and won’t do simple things.
- But it does seem to clear up, when the storm passes.
This is probably the third time, that it’s happened.
Note.
- My left humerus was broken by the school bully.
- I had a stroke in 2011, which affected my left arm.
- If I carry shopping in my left hand, the pulling action on my humerus seems to help.
Any ideas will be gratefully received.
Application Of Control Engineering Principles To The Calculation Of Pharmaceutical Drug Doses
Today, I was asked by an eminent cardiologist to give my opinion on this scientific paper in the Journal of the American Heart Association, which was entitled Personalized Antihypertensive Treatment Optimization With Smartphone‐Enabled Remote Precision Dosing of Amlodipine During the COVID‐19 Pandemic (PERSONAL‐CovidBP Trial).
This was the background to the study.
The objective of the PERSONAL‐CovidBP (Personalised Electronic Record Supported Optimisation When Alone for Patients With Hypertension: Pilot Study for Remote Medical Management of Hypertension During the COVID‐19 Pandemic) trial was to assess the efficacy and safety of smartphone‐enabled remote precision dosing of amlodipine to control blood pressure (BP) in participants with primary hypertension during the COVID‐19 pandemic.
These were the methods and the results.
This was an open‐label, remote, dose titration trial using daily home self‐monitoring of BP, drug dose, and side effects with linked smartphone app and telemonitoring. Participants aged ≥18 years with uncontrolled hypertension (5–7 day baseline mean ≥135 mm Hg systolic BP or ≥85 mm Hg diastolic BP) received personalized amlodipine dose titration using novel (1, 2, 3, 4, 6, 7, 8, 9 mg) and standard (5 and 10 mg) doses daily over 14 weeks. The primary outcome of the trial was mean change in systolic BP from baseline to end of treatment. A total of 205 participants were enrolled and mean BP fell from 142/87 (systolic BP/diastolic BP) to 131/81 mm Hg (a reduction of 11 (95% CI, 10–12)/7 (95% CI, 6–7) mm Hg, P<0.001). The majority of participants achieved BP control on novel doses (84%); of those participants, 35% were controlled by 1 mg daily. The majority (88%) controlled on novel doses had no peripheral edema. Adherence to BP recording and reported adherence to medication was 84% and 94%, respectively. Patient retention was 96% (196/205). Treatment was well tolerated with no withdrawals from adverse events.
These were the conclusions.
Personalized dose titration with amlodipine was safe, well tolerated, and efficacious in treating primary hypertension. The majority of participants achieved BP control on novel doses, and with personalization of dose there were no trial discontinuations due to drug intolerance. App‐assisted remote clinician dose titration may better balance BP control and adverse effects and help optimize long‐term care.
About Myself
I am a Graduate Control Engineer, who graduated from the University of Liverpool in 1968.
I then worked at ICI in Runcorn for eighteen months, before moving to ICI Plastics Division, because of the untimely death of my father-in-law.
One of my tasks at Welwyn, was to look at control algorithms for chemical plants. For this I often used a PACE 231-R analogue computer.

Note.
- These computers could solve up to a hundred simultaneous differential equations at one time.
- They were programmed by wiring the various amplifiers and potentiometers together to simulate the equations.
- There were only a few transistors in these powerful machines, as all electronics were thermionic valves.
- Two of these machines wired together, were used to calculate the trajectories of the Apollo missions.
They were the unsung heroes of bringing Jim Lovell and Apollo 13 home safely.
Determining Control Algorithms
In a typical problem, I would model the a section of a chemical plant and the control system around it.
This would then lead to recommendations, as to the design and operation of the plant, so that it performed as required.
It could be argued that the body of an animal, is a very complicated integrated chemical plant, with a sophisticated control system.
For instance, if sensors around the body, say you are slightly low on fluids, your brain determines you should have a drink.
Many control loops on a chemical plant are controlled by proportional–integral–derivative controllers, which are commonly known as three-term controllers.
This is the first two paragraphs of the Wikipedia entry for three-term controllers.
A proportional–integral–derivative controller (PID controller or three-term controller) is a control loop mechanism employing feedback that is widely used in industrial control systems and a variety of other applications requiring continuously modulated control. A PID controller continuously calculates an error value
PID systems automatically apply accurate and responsive correction to a control function. An everyday example is the cruise control on a car, where ascending a hill would lower speed if constant engine power were applied. The controller’s PID algorithm restores the measured speed to the desired speed with minimal delay and overshoot by increasing the power output of the engine in a controlled manner.
I wouldn’t be surprised that the app in the smartphone used in the PERSONAL‐CovidBP Trial contained a form of three-term controller.
These are some points about three-term control algorithms.
Changing Of External Factors
One that was the villain in a problem, I dealt with, also affects my body – the weather.
I was asked to look at the problem of a chemical reaction, that overheated in hot weather. But the plant operators solved it by better insulation and ventilation of the plant and the standard three-term controller adjusted itself automatically to the new conditions.
After my stroke, I am on Warfarin for life. I test my own INR with a Roche meter and I have noticed that atmospheric pressure affects my INR. I change my deose accordingly, using a simple algorithm, of my own design.
The More You Test The More Precise The Control
If you take the cruise control example used by Wikipedia, speed is monitored continuously, as I hope, it would be if you were driving yourself.
But obviously, in many systems, where you are using an input with discrete values to control a system, you can’t be as precise as the data you collect.
When my son was dying from pancreatic cancer, he was fitted with a morphine pump, that he could adjust himself to dull the immense pain he was enduring.
- His nerves and his brain ascertained the pain level.
- He then adjusted the morphine level.
- He could get very precise control of his pain, because he was measuring it continuously.
But he was only using simple one-term control (proportional).
Derivative Control Can Be Difficult To Get Right And Can Even Go Unstable
Derivative control is mainly to stop overshoot, but sometimes you will find that it can go unstable, so two-term(proportional+integral) controllers will be used.
How I Control My INR
As I said earlier, I am on Warfarin for life and test my INR with a Roche meter.
The NHS typically tests patients about once every six weeks, which in my opinion as a Control Engineer is too infrequent.
I usually test myself a couple of times a week.
But every so often, I evaluate what daily dose gives me an equilibrium INR level of 2.5.
For the last three years, I have found a dose of 3.75 mg keeps me more or less on 2.5.
- As Warfarin comes in 1, 3, 5 and 10 mg. tablets, I alternate 3.5 and 4 mg.
- Warfarin tablets are easily cut in half using a sharp knife.
- I record INR and dose in a spreadsheet.
I have been doing this now for over ten years.
Is This A Unique Property Of Warfarin?
In this time, I have had five medical procedures, where surgeons were worried, that as I was on Warfarin, I might bleed too much.
For the first, which was to remove a lump from my mouth, the private surgeon wanted to charge extra for an anaesthetist. In the end, I asked what INR he wanted and he said 2.1 should be OK!
- So I reduced the Warfarin level and tested every day.
- I judged it correctly and had an INR of 2.1 on the day of the operation.
- The operation went incredibly well and I went home on public transport.
- The lump turned out to be benign.
- I’ve not had another lump.
After the operation, I increased the Warfarin level and tested every day, until it regained a level of 2.5.
On analysing my doses through the date of the operation, I found that the total amount of Warfarin, I didn’t take to reduce my INR to 2.1, was the same as I took to bring it back up again to 2.5.
Is this a unique property of Warfarin?
Since then I’ve had two cataract operations performed in a private hospital, where the NHS paid. Interestingly, they wouldn’t trust my own INR readings, so I had to get my GP to take the measurement.
I’ve also had gallstones removed by endoscopy at the local Homerton NHS hospital.
- For cases like mine, the hospital hire in a surgeon from the posh Wellington private hospital for one day a week, who brings the specialist tools needed.
- I wrote about this in Goodbye To My Gallstones.
- As it was a more serious procedure, I reduced my INR to a requested 1.0.
Interestingly, I still have my gall bladder, but the surgeon put it on notice to behave.
Conclusion
I would totally agree with the conclusion given in the PERSONAL‐CovidBP Trial.
Personalized dose titration with amlodipine was safe, well tolerated, and efficacious in treating primary hypertension. The majority of participants achieved BP control on novel doses, and with personalization of dose there were no trial discontinuations due to drug intolerance. App‐assisted remote clinician dose titration may better balance BP control and adverse effects and help optimize long‐term care.
I would add some conclusions of my own.
- The app used in the PERSONAL‐CovidBP Trial, seems to have had a good algorithm.
- I suspect the app could also be Internet-based.
These are some general conclusions.
- If you are on Warfarin and have access to a Roche meter, it is possible to lower your INR to the value required by a surgeon for an operation or a procedure.
- Since starting to take Warfarin, I have had four operations or procedures, where others would have had anaesthetic or a sedative.
- In those four operations, I was able to go home on public transport. If I still drove a car, I could have driven home afterwards.
- Private hospitals like to use an anesthetist, as it pumps up the bill.
- Avoiding anaesthesia must save hospitals money.
Well designed apps, based on Control Engineering principles, that help the patient take the best dose of a drug will become more common.
The Great Cadaver Shortage: Inside Doctors’ Latest Crisis
The title of this post, is the same as that of this article in The Times.
This is the sub-heading.
Faced with a dwindling supply of fresh bodies to train on, British medical schools are having to turn to America’s low-regulation ‘tissue trade’. Would you donate yours, asks Jenny Kleeman
My late wife, C; left her body to medical science and I may well choose to do the same with my body.
She left her body to St. George’s Medical School, mainly because one of her friend’s mother had done the same and there had been no problems.
Looking back on the nearly twenty years since she died, I remember a few months after her death, there was a multi-faith joint Memorial Service in Southwark Cathedral for all those who’d donated their bodies, in the previous year.
None of my family were or are religious, but I’m sure the service helped our grieving, as it was a very moving and inclusive service, that was the Church of England at its best, with assistance from other faiths.
Perhaps if donation were to be linked to support for the bereaved and perhaps a Memorial Service, this might increase the level of donations.
What sort of affect would it create in a city like Liverpool, if the yearly service alternated around the major places of worship in the city and was well-covered on local media?
Why Don’t Whales Get Cancer? Cracking One Of Medicine’s Greatest Mysteries
The title of this post, is the same as that of this article on The Guardian.
This is the sub-heading.
Understanding why some animals are more susceptible to the disease could lead to improved screening for humans
These are the first three paragraphs
Scientists are homing in on one of medicine’s most baffling mysteries: why some species avoid getting cancers while others are plagued by tumours that shorten their lives.
Whales tend to have low rates of cancer but it is the leading cause of death for dogs and cats. Foxes and leopards are susceptible while sheep and antelopes are not. Bats are also relatively well protected against cancer but not mice or rats. In humans, cancer is a leading cause of death that kills around 10 million people a year.
Even more puzzling is the fact that many huge creatures, including whales and elephants, generally avoid cancer when, instead, they should be at special risk because they possess vast numbers of cells, each of which could trigger a tumour.
The article is definitely a must-read.
A Funny Wet Week
I’ve had a funny few days as regards my health.
Tursday morning, my INR was 2.1.
On Friday night, I wasn’t sleeping very well and got up at three on Saturday morning. But after a couple of mugs of tea, I was feeling a lot better.
I had my usual Saturday morning breakfast in Leon on Moorgate, but I did get slightly confused with my shopping in Marks & Spencer. I put this down to my eyesight having an off day. Is that normal after two cataract operations?
I slept better on Saturday night! But was this because I went to bed before instead of after Match of the Day and then watched it on Sunday morning.
On Sunday morning, I went out to do a bit of shopping, but it was really just to get out and then it was walking in the pouring rain.
Monday was a quiet day, after breakfast in Leon on Moorgate, I wrote for most of the day. My INR was a bit low at 2.2.
Tuesday morning, it was a repeat of Friday night and I got up at four and had a couple of mugs of tea. It was another breakfast in Leon on Moorgate and a visit to M & S. After I returned, I wrote for most of the day, as it was too wet to go outside.
In the afternoon, I started to get a bit unsteady on my feet and even thought about calling 999. But after two mugs of tea and a can of Adnams, I regained my balance and never fell. My blood pressure was fine and the only unusual thing, was that my left food was quite red. But it does this sometimes.
Wednesday was uneventful and I had lunch with a friend at Cote in Sloane Square.
Today, Thursday my INR is down to 2.
I feel OK, but it does seem, that for some reason my INR has tended to slump during the week.
I just wonder if my leaky skin, just lets water out, which surely must lower the INR.
Does my foot go red, as the red blood corpuscles are too big to get through my skin?
